
Abstract
Purpose
To identify pathological features for sample analysis of magnetic resonance imaging-guided vaccum-assisted breast biopsy (MRIgVaBB) to optimize radio pathological correlation and identify discordant benign result.
Material and methods
Databases of two centres were queried to identify MRIgVaBB performed between January 2009 and February 2013. A cohort of 197 women (mean age: 54.5 years (24-77)) with 208 lesions was identified. We retrospectively analyzed all prebiopsy MRI examinations according to the new BI-RADS lexicon, and all biopsy samples to describe the lesion of interest, its interface with the surrounding breast tissue and other associated features.
Results
The malignancy rate was 26.0 % (54/208) with an underestimation rate of 15.67 % (5/32). A visible interface at pathology between a biopsied lesion and the surrounding breast tissue was more frequently identified in mass enhancement compared to NME or focus (p = 0.0003). Regional NME was correlated with a high degree of fibrosis (p = 0.001) and the presence of PASH (p = 0.0007). Linear or segmental NME was correlated with the presence of periductal mastitis (p = 0.0003).
Conclusion
The description of a visible interface between the target lesion and the surrounding tissue is crucial to confirm the correct targeting of an MR mass or a NME.
Key points
• Pathological interface correlated with magnetic resonance mass and focal non-mass enhancement (NME).
• Linear or segmental NME correlated with mastitis or ductal carcinoma in situ.
• Fibrosis and pseudoangiomatous stromal hyperplasia (PASH) are correlated with regional NME.





Similar content being viewed by others


References
Orel SG, Schnall MD (2001) MR imaging of the breast for the detection, diagnosis, and staging of breast cancer. Radiology 220:13–30
Morris EA (2003) Screening for breast cancer with MRI. Semin Ultrasound CT MR 24:45–54
Sardanelli F, Boetes C, Borisch B et al (2010) Magnetic resonance imaging of the breast: recommendations from the EUSOMA working group. Eur J Cancer 46:1296–1316
Sung JS, Lee CH, Morris EA et al (2012) Patient follow-up after concordant histologically benign imaging-guided biopsy of MRI-detected lesions. AJR Am J Roentgenol 198:1464–1469
Li J, Dershaw DD, Lee CH et al (2009) MRI follow-up after concordant, histologically benign diagnosis of breast lesions sampled by MRI-guided biopsy. AJR Am J Roentgenol 193:850–855
Shaylor SD, Heller SL, Melsaether AN et al (2014) Short interval follow-up after a benign concordant MR-guided vacuum assisted breast biopsy - is it worthwhile? Eur Radiol 24:1176–1185
Crystal P, Sadaf A, Bukhanov K et al (2011) High-risk lesions diagnosed at MRI-guided vacuum-assisted breast biopsy: can underestimation be predicted? Eur Radiol 21:582–589
Perlet C, Heywang-Kobrunner SH, Heinig A et al (2006) Magnetic resonance-guided, vacuum-assisted breast biopsy: results from a European multicenter study of 538 lesions. Cancer 106:982–990
Liberman L, Bracero N, Morris E et al (2005) MRI-guided 9-gauge vacuum-assisted breast biopsy: initial clinical experience. AJR Am J Roentgenol 185:183–193
Orel SG, Rosen M, Mies C, Schnall MD (2006) MR imaging-guided 9-gauge vacuum-assisted core-needle breast biopsy: initial experience. Radiology 238:54–61
Han BK, Schnall MD, Orel SG, Rosen M (2008) Outcome of MRI-guided breast biopsy. AJR Am J Roentgenol 191:1798–1804
Perretta T, Pistolese CA, Bolacchi F et al (2008) MR imaging-guided 10-gauge vacuum-assisted breast biopsy: histological characterisation. Radiol Med 113:830–840
Malhaire C, El Khoury C, Thibault F et al (2010) Vacuum-assisted biopsies under MR guidance: results of 72 procedures. Eur Radiol 20:1554–1562
Morris EA, Cornstock CE, Lee CH (2013) ACR BI-RADS Magnetic Resonance Imaging. In: ACR BI-RADS Atlas, Breast Imaging REporting and Data System, 5th ed. American College of Radiology, Reston
Lakhani SR, Schnitt SJ, Hoon Tan P, van de Vijver MJ (2011) WHO classification of Tumours of the breast. Switzerland
Parikh J, Tickman R (2005) Image-guided tissue sampling: where radiology meets pathology. Breast J 11:403–409
Lehman CD, Deperi ER, Peacock S et al (2005) Clinical experience with MRI-guided vacuum-assisted breast biopsy. AJR Am J Roentgenol 184:1782–1787
Liberman L, Morris EA, Dershaw DD et al (2003) Ductal enhancement on MR imaging of the breast. AJR Am J Roentgenol 181:519–525
Thomassin-Naggara I, Trop I, Chopier J, et al. (2011) Nonmasslike enhancement at breast MR imaging: the added value of mammography and US for lesion categorization
Acknowledgments
The scientific guarantor of this publication is Isabelle Thomassin-Naggara.
Isabelle Thomassin-Naggara declares a relationship with two companies: General Electric (Honoraries for speaking, travel congress payment) and Olea Medical (Consulting). These relationships have no influence on the design or any result of this article. The other authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. One of the authors has significant statistical expertise. Institutional Review Board approval was obtained. Written informed consent was not required for this study because our institutional ethics committees approved the study and granted a waiver of informed consent. Methodology: retrospective, observational, multicenter study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
1A
Supplemental 1: Additional histological features. 1A: Diffuse associated features: Lobular atrophy 1. Presence. 2. Absence (HES × 2.5) (JPEG 101 kb)
2A
(JPEG 90 kb)
1B
Supplemental 1: Additional histological features. 1B: Diffuse associated features: Cellularity 1. Low 2. moderate or high (HES × 2.5) (JPEG 120 kb)
2B
(JPEG 134 kb)
1C
Supplemental 1: Additional histological features. 1C: Diffuse associated features: Relative proportion of fibrous and adipose tissue 1.90 %/10 % and 2. 10 %/90 % (Whole slide scanning) (JPEG 31 kb)
2C
(JPEG 15 kb)
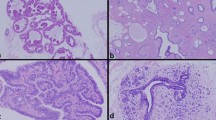
1D
Supplemental 1: Additional histological features. 1D: Focal associated features: Periductal mastitis. In that case, periductal mastitis is associated with ductal ectasia (HES × 2.5) (JPEG 86 kb)
1E
Supplemental 1: Additional histological features. 1E: Focal associated features: PASH (HES × 2.5 and insert HES × 10) (JPEG 157 kb)
1F
Supplemental 1: Additional histological features. 1F: Focal associated features: Apocrine metaplasia (HES × 10) (JPEG 86 kb)
1G
Supplemental 1: Additional histological features. 1G: Interface between lesion and surrounding breast parenchyma. 1. No visible interface between adenosis with usual ductal hyperplasia and surrounding breast parenchyma. 2. Visible interface between fibroadenoma and surrounding adipose breast parenchyma) (HES × 2.5) (JPEG 156 kb)
2G
(JPEG 140 kb)
2A
Supplemental 2: At MR, this lesion was described as a mass whereas no nodule was found at pathology. However a visible interface between the target lesion and the surrounding tissue was found allowing a good radiopathological correlation. (HES × 2.5). (JPEG 10 kb)
2B
(JPEG 147 kb)
Rights and permissions
About this article

Cite this article
Dratwa, C., Jalaguier-Coudray, A., Thomassin-Piana, J. et al. Breast MR biopsy: Pathological and radiological correlation. Eur Radiol 26, 2510–2519 (2016). https://doi.org/10.1007/s00330-015-4071-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-015-4071-y