
Abstract
Objectives
To determine whether fast scanned MRI using a 1.5-T scanner is a reliable method for the detection and characterization of acute ischemic stroke in comparison with conventional MRI.
Methods
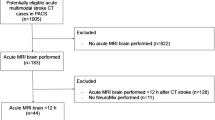
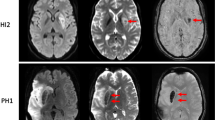
From May 2015 to June 2016, 862 patients (FLAIR, n = 482; GRE, n = 380; MRA, n = 190) were prospectively enrolled in the study, with informed consent and under institutional review board approval. The patients underwent both fast (EPI-FLAIR, ETL-FLAIR, TR-FLAIR, EPI-GRE, parallel-GRE, fast CE-MRA) and conventional MRI (FLAIR, GRE, time-of-flight MRA, fast CE-MRA). Two neuroradiologists independently assessed agreements in acute and chronic ischemic hyperintensity, hyperintense vessels (FLAIR), microbleeds, susceptibility vessel signs, hemorrhagic transformation (GRE), stenosis (MRA), and image quality (all MRI), between fast and conventional MRI. Agreements between fast and conventional MRI were evaluated by generalized estimating equations. Z-scores were used for comparisons of the percentage agreement among fast FLAIR sequences and fast GRE sequences and between conventional and fast MRA.
Results
Agreements of more than 80% were achieved between fast and conventional MRI (ETL-FLAIR, 96%; TR-FLAIR, 97%; EPI-GRE, 96%; parallel-GRE, 98%; fast CE-MRA, 86%). ETL- and TR-FLAIR were significantly superior to EPI-FLAIR in the detection of acute ischemic hyperintensity and hyperintense vessels, while parallel-GRE was significantly superior to EPI-GRE in the detection of susceptibility vessel sign (p value < 0.05 for all). There were no significant differences in the other scores and image qualities (p value > 0.05).
Conclusions
Fast MRI at 1.5 T is a reliable method for the detection and characterization of acute ischemic stroke in comparison with conventional MRI.
Key Points
• Fast MRI at 1.5 T may achieve a high intermethod reliability in the detection and characterization of acute ischemic stroke with a reduction in scan time in comparison with conventional MRI.





Similar content being viewed by others

Abbreviations
- CT:
-
Computed tomography
- DWI:
-
Diffusion-weighted imaging
- EPI:
-
Echo-planar imaging
- EPI-FLAIR:
-
FLAIR using echo-planar imaging
- EPI-GRE:
-
GRE using echo-planar imaging
- ETL-FLAIR:
-
FLAIR with increased echo train length
- Fast CE-MRA:
-
Contrast-enhanced MRA with increased acceleration factor and slice thickness
- FLAIR:
-
Fluid-attenuated inversion recovery
- GRE:
-
Gradient echo T2*-weighted imaging
- MRA:
-
Magnetic resonance angiography
- MRI:
-
Magnetic resonance imaging
- Parallel-GRE:
-
GRE with increased acceleration factor
- PWI:
-
Perfusion-weighted imaging
References
Kim BJ, Kang HG, Kim H-J et al (2014) Magnetic resonance imaging in acute ischemic stroke treatment. J Stroke 16:131
Nael K, Khan R, Choudhary G et al (2014) Six-minute magnetic resonance imaging protocol for evaluation of acute ischemic stroke: pushing the boundaries. Stroke 45:1985–1991
Warach S, Chien D, Li W, Ronthal M, Edelman RR (1992) Fast magnetic resonance diffusion-weighted imaging of acute human stroke. Neurology 42:1717–1723
Chalela JA, Kidwell CS, Nentwich LM et al (2007) Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet 369:293–298
Albers GW, Thijs VN, Wechsler L et al (2006) Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol 60:508–517
Davis SM, Donnan GA, Parsons MW et al (2008) Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol 7:299–309
Tong DC, Albers GW, Yenari MA, Marks MP (1999) A standardized MRI stroke protocol: comparison with CT in hyperacute intracerebral hemorrhage. Stroke 30:1974–1981
Badhiwala JH, Nassiri F, Alhazzani W et al (2015) Endovascular thrombectomy for acute ischemic stroke: a meta-analysis. JAMA 314:1832–1843
Lin Z, Guo Z, Qiu L, Yang W, Lin M (2016) The applied research of MRI with ASSET-EPI-FLAIR combined with 3D TOF MRA sequences in the assessment of patients with acute cerebral infarction. Acta Radiol 57:1515–1523
Korogi Y, Sugahara T, Shigematsu Y et al (1999) Ultrafast FLAIR imaging with single-shot echo-planar technique in evaluation of intracranial lesions. Comput Med Imaging Graph 23:119–126
Meshksar A, Villablanca JP, Khan R, Carmody R, Coull B, Nael K (2014) Role of EPI-FLAIR in patients with acute stroke: a comparative analysis with FLAIR. AJNR Am J Neuroradiol 35:878–883
Tomura N, Kato K, Takahashi S et al (2002) Comparison of multishot echo-planar fluid-attenuated inversion-recovery imaging with fast spin-echo fluid-attenuated inversion-recovery and T2-weighted imaging in depiction of white matter lesions. J Comput Assist Tomogr 26:810–814
Gai ND, Butman JA (2015) Reduced scan time 3D FLAIR using modulated inversion and repetition time. J Magn Reson Imaging 41:1440–1446
JM UK-I, Trivedi RA, Graves MJ et al (2005) Utility of an ultrafast magnetic resonance imaging protocol in recent and semi-recent strokes. J Neurol Neurosurg Psychiatry 76:1002–1005
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP (2007) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335:806–808
Ebinger M, Galinovic I, Rozanski M, Brunecker P, Endres M, Fiebach JB (2010) Fluid-attenuated inversion recovery evolution within 12 hours from stroke onset: a reliable tissue clock? Stroke 41:250–255
Petkova M, Rodrigo S, Lamy C et al (2010) MR imaging helps predict time from symptom onset in patients with acute stroke: implications for patients with unknown onset time. Radiology 257:782–792
Yoshioka K, Ishibashi S, Shiraishi A, Yokota T, Mizusawa H (2013) Distal hyperintense vessels on FLAIR images predict large-artery stenosis in patients with transient ischemic attack. Neuroradiology 55:165–169
Wardlaw JM, Smith EE, Biessels GJ et al (2013) Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 12:822–838
Arnould M-C, Grandin CB, Peeters A, Cosnard G, Duprez TP (2004) Comparison of CT and three MR sequences for detecting and categorizing early (48 hours) hemorrhagic transformation in hyperacute ischemic stroke. AJNR Am J Neuroradiol 25:939–944
Vert C, Parra-Farinas C, Rovira A (2017) MR imaging in hyperacute ischemic stroke. Eur J Radiol. https://doi.org/10.1016/j.ejrad.2017.06.013
Funding
This study has received funding by the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea (HI12C1847).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Sang Joon Kim.
Conflict of interest
The authors declare that they have no conflict of interest.
Statistics and biometry
One of the authors (S Baek) has significant statistical expertise.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• Prospective
• Diagnostic study
• Performed at one institution
Electronic supplementary material
ESM 1
(DOCX 997 kb)
Rights and permissions
About this article

Cite this article
Chung, M.S., Lee, J.Y., Jung, S.C. et al. Reliability of fast magnetic resonance imaging for acute ischemic stroke patients using a 1.5-T scanner. Eur Radiol 29, 2641–2650 (2019). https://doi.org/10.1007/s00330-018-5812-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5812-5