
Abstract
Purpose
To determine the earliest optimal timing for assessment of early response following radioimmunotherapy in non-Hodgkin lymphoma patients using FDG-PET/CT.
Methods
FDG-PET/CT was performed prior to treatment (PET1), at 2 (PET2) weeks, and at 6 (PET3) weeks after 90Y-ibritumomab radioimmunotherapy in 55 patients. Response was evaluated based on the Deauville 5-point scale and Lugano criteria as well as semiquantitative analysis and compared with progression-free survival (PFS).
Results
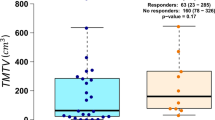
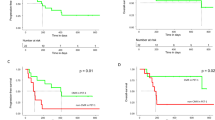
PET 2 showed complete metabolic response (CMR), partial metabolic response (PMR), stable metabolic disease (SMD), and progressive metabolic disease (PMD) in 33, 13, 6, and 3 patients, respectively, while PET 3 in 41, 8, 3, and 3 patients, respectively. Mean SUVmax of 168 target lesions decreased over time (PET1, 2, 3; 5.58 ± 2.58, 1.87 ± 1.78, 1.75 ± 2.25, respectively). Progression or recurrence after a median of 12.6 months (range 2.6–72.0 months) was seen in 44 patients. Patients with CMR or metabolic response (CMR + PMR) on PET2 showed significantly longer PFS as compared to those who did not (p = 0.00028 and p = 0.029, respectively). A similar significant difference was observed based on PET3 (p = 0.00013 and p = 0.017, respectively). The same trend was observed when analyzing only the subgroup of patients with follicular lymphoma (N = 43/55) (p < 0.0001).
Conclusion
Use of FDG-PET/CT findings with Lugano criteria for assessing early response to radioimmunotherapy after 6 weeks allowed for accurate evaluation and prognostic stratification, though scanning after 2 weeks was too soon to precisely evaluate response.
Key Points
• The optimal timing of FDG-PET/CT to obtain a suitable tool for assessment of response after 90 Y-ibritumomab radioimmunotherapy of lymphoma has not yet been defined.
• Assessment after 6 weeks by FDG-PET/CT using the Lugano criteria accurately evaluates treatment response and prognosis.
• FDG-PET/CT performed 2 weeks after radioimmunotherapy is too early as it significantly misses objective responses.






Similar content being viewed by others
Abbreviations
- CMR:
-
Complete metabolic response
- FDG:
-
18F-fluorodeoxyglucose
- FOV:
-
Field of view
- MALT:
-
Mucosa-associated lymphoid tissue
- PET/CT:
-
Positron emission tomography/computed tomography
- PFS:
-
Progression-free survival
- PMD:
-
Progressive metabolic disease
- PMR:
-
Partial metabolic response
- SMD:
-
Stable metabolic disease
- SUVmax :
-
Maximum standardized uptake value
- VOI:
-
Volume of interest
References
Wagner HN Jr, Wiseman GA, Marcus CS et al (2002) Administration guidelines for radioimmunotherapy of non-Hodgkin's lymphoma with (90)Y-labeled anti-CD20 monoclonal antibody. J Nucl Med 43:267–272
Witzig TE, Gordon LI, Cabanillas F et al (2002) Randomized controlled trial of yttrium-90-labeled ibritumomab tiuxetan radioimmunotherapy versus rituximab immunotherapy for patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin’s lymphoma. J Clin Oncol 20:2453–2463
Kaminski MS, Tuck M, Estes J et al (2005) 131I-tositumomab therapy as initial treatment for follicular lymphoma. N Engl J Med 352:441–449
Illidge TM, Mayes S, Pettengell R et al (2014) Fractionated 90Y-ibritumomab tiuxetan radioimmunotherapy as an initial therapy of follicular lymphoma: an international phase II study in patients requiring treatment according to GELF/BNLI criteria. J Clin Oncol 32:212–218
McQuillan AD, Macdonald WB, Turner JH (2015) Phase II study of first-line 131I-rituximab radioimmunotherapy in follicular non-Hodgkin lymphoma and prognostic 18F-fluorodeoxyglucose positron emission tomography. Leuk Lymphoma 56:1271–1277
Bodet-Milin C, Kraeber-Bodéré F, Dupas B et al (2008) Evaluation of response to fractionated radioimmunotherapy with 90Y-epratuzumab in non-Hodgkin's lymphoma by 18F-fluorodeoxyglucose positron emission tomography. Haematologica 93:390–397
Jacene H, Crandall J, Kasamon YL et al (2017) Initial experience with tositumomab and I-131-labeled tositumomab for treatment of relapsed/refractory Hodgkin lymphoma. Mol Imaging Biol 19:429–436
Lim I, Park JY, Kang HJ et al (2013) Prognostic significance of pretreatment 18F-FDG PET/CT in patients with relapsed/refractory B-cell non-Hodgkin's lymphoma treated by radioimmunotherapy using 131I-rituximab. Acta Haematol 130:74–82
Torizuka T, Zasadny KR, Kison PV, Rommelfanger SG, Kaminski MS, Wahl RL (2000) Metabolic response of non-Hodgkin’s lymphoma to 131I-anti-B1 radioimmunotherapy: evaluation with FDG PET. J Nucl Med 41:999–1005
Kaneko K, Choi I, Nakagawa M, Shinozaki K, Uike N (2014) Does tumoral 111In-ibritumomab accumulation correlate with therapeutic effect and outcome in relapsed or refractory low-grade B-cell lymphoma patients undergoing 90Y-ibritumomab radioimmunotherapy? Eur Radiol 24:3191–3198
Cheson BD, Fisher RI, Barrington SF et al (2014) Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 32:3059–3068
Jacene HA, Filice R, Kasecamp W, Wahl RL (2009) 18F-FDG PET/CT for monitoring the response of lymphoma to radioimmunotherapy. J Nucl Med 50:8–17
Storto G, De Renzo A, Pellegrino T et al (2010) Assessment of metabolic response to radioimmunotherapy with 90Y-ibritumomab tiuxetan in patients with relapsed or refractory B-cell non-Hodgkin lymphoma. Radiology 254:245–252
Lopci E, Santi I, Derenzini E et al (2010) FDG-PET in the assessment of patients with follicular lymphoma treated by ibritumomab tiuxetan Y 90: multicentric study. Ann Oncol 21:1877–1883
Grgic A, Nestle U, Scheidhauer K et al (2011) Retrospective web-based multicenter evaluation of 18F-FDG-PET and CT derived predictive factors. Radioimmunotherapy with yttrium-90-ibritumomab tiuxetan in follicular non Hodgkin’s lymphoma. Nuklearmedizin 50:39–47
Kesavan M, Boucek J, MacDonald W, McQuillan A, Turner JH (2017) Imaging of early response to predict prognosis in the first-line management of follicular non-Hodgkin lymphoma with Iodine-131-rituximab radioimmunotherapy. Diagnostics (Basel) 7
De Saint-Hubert M, Devos E, Ibrahimi A, Debyser Z, Mortelmans L, Mottaghy FM (2012) Bioluminescence imaging of therapy response does not correlate with FDG-PET response in a mouse model of Burkitt lymphoma. Am J Nucl Med Mol Imaging 2:353–361
Brepoels L, De Saint-Hubert M, Stroobants S et al (2010) Dose-response relationship in cyclophosphamide-treated B-cell lymphoma xenografts monitored with [18F]FDG PET. Eur J Nucl Med Mol Imaging 37(9):1688–1695
Song S, Xiong C, Lu W, Ku G, Huang G, Li C (2013) Apoptosis imaging probe predicts early chemotherapy response in preclinical models: a comparative study with 18F-FDG PET. J Nucl Med 54:104–110
Acknowledgements
We thank the editors of European Radiology and those who reviewed this article.
Funding
We declare no financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Koichiro Yamakado.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Informed consent was obtained from each patient after the procedure details were fully explained.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• prospective
• diagnostic or prognostic study
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kitajima, K., Okada, M., Kashiwagi, T. et al. Early evaluation of tumor response to 90Y-ibritumomab radioimmunotherapy in relapsed/refractory B cell non-Hodgkin lymphoma: what is the optimal timing for FDG-PET/CT?. Eur Radiol 29, 3935–3944 (2019). https://doi.org/10.1007/s00330-019-06134-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-019-06134-7