High resolution diffusion weighted-magnetic resonance imaging for risk stratification in intraductal papillary mucinous neoplasia
by Omar Kamal, Georgios Kaissis, Christoph Zöllner, Marianne Reiser, Helmut Friess, Roland Schmid, Hana Algül, Wilko Weichert, Dimitrios Karampinos, Rickmer Braren (rbraren@tum.de)
Dear Editor,
We would like to raise attention to the potential need for a revisit of suggested imaging protocols for intraductal papillary mucinous neoplasms (IPMN) in light of the progress in abdominal MRI techniques exemplified a poignant case from our specialist referral center.
IPMNs are a subgroup of pre-neoplastic pancreatic lesions, which can be morphologically subclassified into main-duct (MD), branch-duct (BD) or mixed-type (MT). Their rising incidence is attributed to increased discovery and reporting in cross-sectional imaging [1]. Because of their malignant potential, resection is recommended upon diagnosis for MD- and MT-IPMNs, characterized by a main pancreatic duct (MPD) diameter of ≥ 10 mm. The management of BD-IPMNs is more complex, as their incidence of malignancy i.e. presentation of an IPMN-derived or (less frequently), a concomitant PDAC [2, 3], is lower. Surgical removal is recommended for BD-IPMN only when specific high risk features are present (jaundice, contrast-agent (CA) affine nodule ≥ 5 mm or MPD diameter ≥ 10 mm) [4, 5]. For non-surgical candidates, continued surveillance is recommended. Specifically, the revised Fukuoka guidelines define worrisome features (i.e. cyst diameter ≥ 3 cm at diagnosis or a > 5 mm growth within 2 years, thickened cyst walls, enhancing nodules < 5 mm/ enhancing septations, MPD diameter of 5-9 mm with distal atrophy, lymphadenopathy) which should prompt further work-up by endoscopic ultrasound (EUS) and, if indicative of malignancy (i.e. enhancing nodule > 5 mm, MPD involvement), surgical removal. Continued surveillance is suggested at varying intervals depending on BD-IPMN diameter, ranging from 6 months initially followed by 2-year intervals (< 1 cm) to 3-6 months intervals (> 3 cm). Also, in smaller lesions (up to 2 cm), computed tomography (CT) or magnetic resonance imaging (MRI) may be used, whereas larger lesions (> 2cm) require MRI or EUS [4]. Similarly, the European evidence-based guidelines on pancreatic cystic neoplasms recommend BD-IPMN patient surveillance in the absence of absolute (solid mass, jaundice, enhancing mural nodule ≥ 5 mm, MPD diameter ≥ 10 mm) or relative (> 5 mm growth in 1 year, MPD diameter 5-9.9 mm, cyst diameter ≥ 4 cm, enhancing nodule < 5 mm) indications for surgery at 6 months initially (for 1 year) and subsequently, at yearly intervals [5].
Guidelines must rely on published evidence [4, 5]. However, rapid technical developments with a rising availability of 3T field MRI and advanced pulse sequence techniques (i.e. reduced field of view diffusion weighted imaging [rFOV DWI], compressed sensing) in abdominal imaging [6–8] have only very recently resulted in significantly improved image quality and diagnostic accuracy in the characterization of pancreatic lesions including IPMNs [9] compared to older data [10–14]. In addition, the recommendation for repeated administrations of gadolinium-based contrast agents (CA) and associated potential complications (i.e. nephrogenic systemic fibrosis, gadolinium deposition) [15, 16] should be critically reviewed in an aging population with potentially reduced kidney function in view of the requirement for long-term follow-up, since older patients might be at increased risk for these complications [11, 12].
The application of diffusion-weighted MRI (DWI), as an imaging technique without the need for CA administration has been investigated in the diagnosis and stratification of IPMN. The DWI-derived apparent diffusion coefficient (ADC) has shown high diagnostic accuracy as a quantitative marker for high risk IPMNs [17-19] with a reported sensitivity for the detection of malignancy in IPMN of 76-77% [18, 19]. Hitherto, the implementation of DWI has been hampered by its lower spatial resolution and signal to noise ratio compared to T1w, T2w and magnetic resonance cholangiopancreaticography (MRCP) images [17], as well as its susceptibility to motion artifacts. Recently, high resolution (rFOV) DWI has been developed, achieving higher image resolution with fewer artifacts and without increasing scan time. It has shown improved image quality in the examination of the pancreas [6–8]. At our institution, we employ a rFOV DWI sequence as part of the contrast free MRI protocol in IPMN surveillance.
The following case highlights the potential advantage of rFOV DWI in risk stratification of IPMNs, as a robust and time- efficient sequence that may obviate contrast enhanced scans: A 78 years old woman was referred to our clinic with multiple pancreatic cystic lesions that were discovered incidentally in routine abdominal ultrasonography. CA 19-9 serum levels were normal. In-house 3T MRI consisting of T2w (3 mm slice thickness, 1:19 min scan time), single breath-hold 3D MRCP (1.0×1.0x2.0 mm, 17.5 s scan time) and rFOV DWI sequences (2.5×2.5×3.0 mm, 3:18 min scan time) revealed multiple BD-IPMNs. The largest BD-IPMN with a diameter of 10 mm was identified in the pancreatic head region and exhibited a focal diffusion restriction of 3 mm, visualized only in the rFOV DWI, prompting further diagnostic work-up by EUS. The lesion exhibited reduced shear stress and perfusion in EUS and a biopsy was taken, confirming the diagnosis of a high grade IPMN. Surgical resection was subsequently performed, and pathological evaluation revealed multiple IPMNs of the pancreato-biliary type, low to high grade with the pancreatic head lesion and a small area of focal transition to invasive adenocarcinoma (G1), less likely concomitant PDAC.
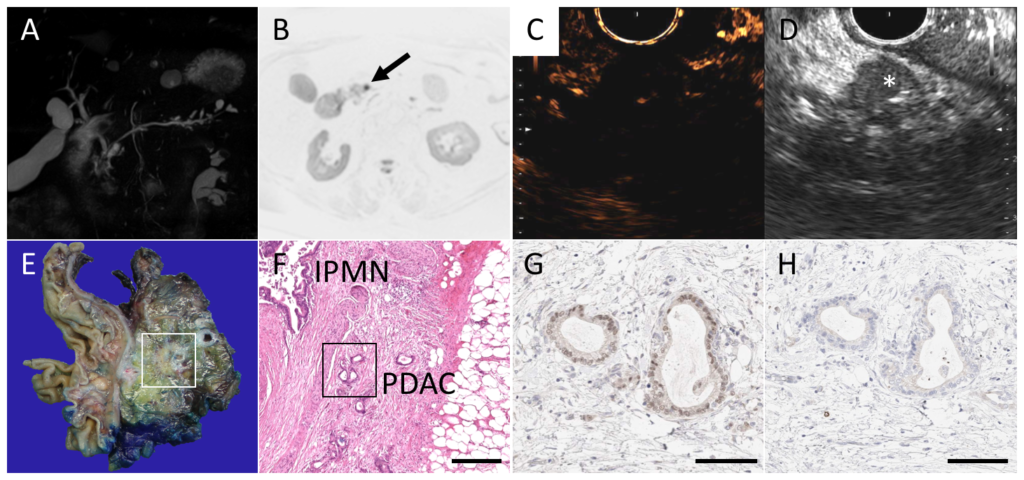
Branch-duct IPMN of the pancreatic head region with carcinoma. A Maximum intensity projection (MIP) of the 3D MRCP dataset showing multiple side branch IPMNs. B B600 image from the rFOV DWI with focal diffusion restriction (arrow). C and D Video still of venous phase CE and corresponding b-mode endoscopic ultrasound showing a hypovascular mass (asterisk). E Photograph of an axial slice of the Whipple resection specimen and photomicrographs of the corresponding (F) H&E, (G) cytokeratin 81 and (H) hepatocyte nuclear factor 1A stainings, showing IPMN and non-basal like carcinoma. Bar in F equals 500µm; bar in G and H equals 100µm.
BD-IPMN are pre-neoplastic lesions with a high incidence, but low frequency of transition to carcinoma or concomitant PDAC. Considering the devastating prognosis of pancreatic cancer, BD-IPMN require close monitoring. The optimal method and intervals for surveillance are a matter of ongoing discussion. EUS is an excellent screening tool enabling immediate cell/tissue sampling for the definitive cytological assessment of suspicious lesions. However, EUS is an invasive procedure with potential risks, and often unpopular with patients [5]. In addition, pancreatic tail lesions can be difficult to visualize [20]. Therefore, MRI is the de facto standard non-invasive imaging tool for IPMN surveillance [4, 5].
Based on the European evidence-based guidelines on pancreatic neoplasms [5], intensive surveillance (i.e. next imaging at 6 month by MRI or EUS) would have been recommended for our patient, as she presented with a new onset diabetes mellitus. Similarly, the revised Fukuoka guidelines for management of IPMN of the pancreas [4], would have recommended CT or MRI follow up at 6 month for our patient. The case presented here questions current guidelines in some aspects: the pancreatic head BD-IPMN had a diameter of 10 mm, which would have qualified it for a CT and no further measures, contrast-enhanced EUS revealed a hypovascular tumor, that would not have been difficult to visualize on CE-MRI, and rFOV DWI (not explicitly recommended as part of a dedicated MRI protocol), was able to visualize the lesion clearly.
In our case, the rFOV b600 image revealed significant diffusion restriction of the nodular lesion in the pancreatic head, not evident in full FOV (fFOV) b600 DWI, attributable to the higher resolution and reduced susceptibility to partial volume effects of the rFOV sequence. The spatial resolution advantage of rFOV DWI in pancreatic imaging is well documented. Ma et al. and Kim et al. have compared rFOV DWI to fFOV DWI and found significant qualitative advantages of rFOV DWI, while retaining stability regarding the absolute ADC values compared to fFOV DWI [9, 14]. Kim et al. furthermore reported rFOV DWI to be superior in smaller lesions (< 1 cm) like the lesion reported in our case [14].
We therefore believe that DWI-MRI is insufficiently considered in pancreatic imaging in general in in particular in the management of BD-IPMN. Technical advances in sequence and hardware design, as demonstrated here, should prompt the evaluation of rFOV DWI in further studies.Prospective studies are required to determine its accuracy. The integration of DWI and in particular rFOV DWI into current guidelines should be considered.